

Did you hear?
Customized dentistry with PreViser is here.
Forget a one size fits all dental treatment plan. With PreViser you get a customized treatment plan based on your oral health needs! Does your dental benefits plan partner with PreViser? If so, you may unlock additional preventive benefits!
Take charge of your oral health by visiting an enrolled PreViser provider. Healthy smiles lead to healthy bodies.

Know your scores

Benefits of the report
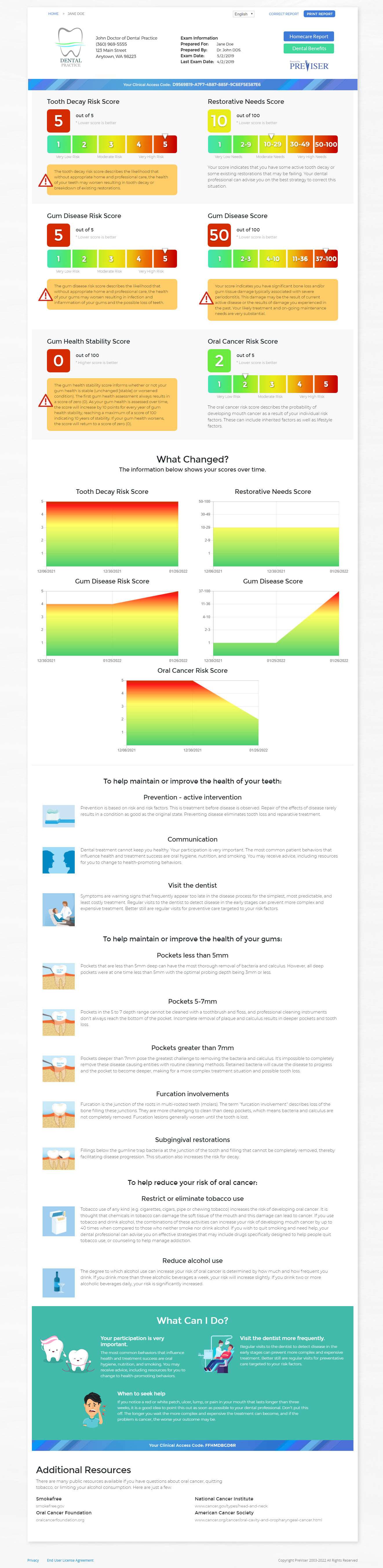
The PreViser report makes it easy to understand where your oral health is today and tomorrow.

What the scores mean
Scores are everywhere because they help us set goals. The PreViser scores tell you where your oral health is today and how to improve it for tomorrow.

Intervention leads to prevention
By implementing preventive treatment, future oral diseases are eliminated. No more dental diseases? Yes please!

We're a team
PreViser communicates your oral health scores so you, your dentist, and insurance company are all working toward the same goal, healthier smiles.
{kind=link}
Perks to the Patient
Knowledge is Power
Know the score. Your oral health score that is. High risk today? No problem with PreViser! Take control of your oral health destiny.
One Size Does Not Fit All
No two patients are the same. Oral health benefits and treatment plans designed just for you.

Oral Health is Health
Research shows oral health is connected to overall health. And why wouldn’t it be? Your mouth is part of your body. Healthy smile. Healthy body.
Help eliminate oral diseases.
Spread the word!
Is your dentist enrolled in PreViser? If not, send a referral.
Having trouble locating a dentist near you? Your current dental provider can sign up here.